
From the 1Graduate School, Tianjin University of Traditional Chinese Medicine, 2Department of Traditional Chinese Medicine, Tianjin First Central Hospital, 3School of Health Sciences and Engineering, Tianjin University of Traditional Chinese Medicine, Tianjin, China and 4Crawford School of Public Policy, Asia and Pacific College, Australian National University, Canberra, ACT, Australia
Background: Physical exercise is an important part of hypertension management. The impact of different training styles and durations of tai chi on essential hypertension has not been evaluated to date.
Objective: To analyse the influence of tai chi on blood pressure and related risk factors in patients with essential hypertension.
Methods: A systematic review to assess the existing literature on the impact of tai chi in patients with essential hypertension. Randomized controlled trials were identified in Chinese and English databases to study the impact of tai chi on essential hypertension. Two reviewers selected studies independently of each other. Qualified trials were selected and their methodological quality critically evaluated.
Results: Thirteen trials were included in the analysis. Following tai chi there was a significant difference between intervention and control groups with regard to change in systolic blood pressure (SBP) (weighted mean difference = −6.58, 95% confidence interval (95% CI) (−8.14, −5.02), p = 0.005) and diastolic blood pressure (DBP) (standardized mean difference = −0.57, 95% CI (−0.77, −0.37), p < 0.0001). Taking into account the subgroup analyses, the combined results showed that 24-movement or yang-style tai chi significantly reduced both systolic and diastolic blood pressure over a period ≤ 12 weeks or > 12 weeks in all studies. However, other styles of tai chi did not significantly reduce systolic or diastolic blood pressure after a duration ≤ 12 weeks.
Conclusion: Tai chi is an effective physical exercise in treating essential hypertension compared with control interventions. Different training durations and styles have different effects. Further randomized controlled trials are needed into the use of tai chi for the treatment and prevention of essential hypertension and other related chronic diseases.
Key words: tai chi; essential hypertension; mind–body exercise; risk factor.
Accepted Apr 15, 2020; Epub ahead pf print Apr 27, 2020
J Rehabil Med 2020; 52: jrm00057
Correspondence address: Hongwu Wang, School of Health Sciences and Engineering, Tianjin University of Traditional Chinese Medicine, Tianjin 301617, China. E-mail: tjwanghw55@163.com
Physical exercise is an important part of hypertension management. The impact of different training styles and durations of tai chi on essential hypertension has not been evaluated to date. The aim of this systematic review was to assess the existing literature on the impact of tai chi in patients with essential hypertension.
With the rapid development of society, people’s diets and living habits have undergone great changes. Increased intake of high-protein and high-fat food, irregular rest and reduced exercise have led to a sharp increase in the number of worldwide patients with hypertension (1, 2). Essential hypertension is a clinical syndrome characterized by increased systemic arterial pressure. The syndrome remains a major threat to public health (3). The prevalence of hypertension is 37.3% in developed countries and 22.9% in developing countries. Worldwide, 25% of adults have high blood pressure (BP), and this proportion is expected to rise to 29% by 2025 (4). Among the population with hypertension, more than 90% have essential hypertension, which makes this type of hypertension a major global chronic non-communicable disease without a secondary cause (5). As an important aspect of hypertension care, lifestyle management, including self-management, physical activity, and nutrition, has attracted increasing attention (6). Physical activity is an important part of hypertension management planning and plays a specific role in the management of BP and prevention of complications in patients with essential hypertension (7). The European Society of Hypertension (ESH) suggests that patients with essential hypertension should increase their physical activity to increase flexibility, muscle strength and balance (6).
Tai chi is used as a physical and mental therapy. It originated from Chinese martial arts and has been widely practised for centuries (8). In modern times, tai chi is used as a form of movement to improve body consciousness and balance (9). It is considered a pleasurable activity that combines meditation with gentle movements (10). A growing body of research has shown that tai chi strengthens the joints, modulates pressure receptors in the aortic arch and carotid sinus, and has a role in lowering BP and expanding the coronary arteries (11–13).
Traditional Chinese exercise can effectively reduce systolic blood pressure (SBP) and diastolic blood pressure (DBP), thereby improving symptoms in patients with cardiovascular disease (14). Some studies have shown that tai chi can reduce the occurrence of cardiovascular risk factors and improve the health of cardiovascular patients (15). However, studies have also shown that tai chi does not reduce BP and risk factors in patients with essential hypertension. In view of the differences in the current studies, a comprehensive and systematic evaluation of the effects of tai chi on BP control and risk factors in patients with essential hypertension is necessary.
The aim of this systematic review was to evaluate the effects of tai chi on BP and risk factors in patients with essential hypertension and to determine the effects of different styles of tai chi and intervention durations on these patients.
Research strategy
PubMed, Cochrane Library, Embase, China National Knowledge Infrastructure (CNKI), VIP Database for Chinese Technical Periodicals (VIP), and Wanfang databases were searched for studies published before December 2019. The search terms were: BP, hypertension, hypertensive, primary hypertension, essential hypertension, tai chi, and randomized controlled trials (RCTs). Two independent reviewers selected and screened all results and, in cases where they disagreed, a third reviewer was asked for advice. The review applied the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement guidelines (16).
Eligibility criteria
Inclusion criteria for this systematic review were: (i) randomized controlled trial (RCT) design related to the therapeutic effect of tai chi; (ii) human subjects were recruited; (iii) tai chi exercise was included as the main intervention in the experimental group and was compared with a usual care or standard treatment control condition; and (iv) at least one BP parameter was reported and data including the mean and standard deviation of each group at baseline and post-intervention, along with the number of participants in each group, were obtainable.
Exclusion criteria were: (i) duplicate publications; (ii) non-intervention designs (such as case-control studies, cohort studies cross-sectional studies, case reports and experiences, theory research, and reviews); and (iii) non-clinical tests and animal experiments.
Data extraction
Two review authors independently screened the literature using the predetermined inclusion criteria and extracted data from the trials. The following information was extracted: participant characteristics, intervention and outcome data, adverse effects, and methodological quality. Any disagreements about the data extracted from the included studies were resolved by consensus, and a third review author was consulted if disagreements persisted.
Risk of bias assessment
The risk of study bias was assessed using the Cochrane Handbook for Systematic Reviews. Risk of bias was evaluated with regard to the following aspects: generating random sequences, allocation of hidden methods, application of the blinding
method, incomplete results, selective reporting of results, and other bias. Funnel diagrams were used to detect publication bias.
Statistical analysis
Extracting and merging data. The Cochrane Collaboration’s Review Manager 5.3 software was used to extract the relevant dichotomous or continuous data from the literature for analysis. Risk ratios (RRs) were calculated for dichotomous data, and mean differences (MDs) and standard deviations (SDs) were calculated for continuous variables. The corresponding 95% confidence intervals (95% CI) and forest plots were used in both cases. The meta-analysis used SD values when the data were in the same unit. When the data were in different units, a conversion was performed. The χ2 and I2 (inconsistency) tests were used to detect heterogeneity. A p-value < 0.10 or I2 > 50% indicated that there was significant heterogeneity. The fixed-effect model was used when p > 0.10 and I2 < 50%, and the random-effect model was used when p < 0.10 or I2 ≥50%.
Data conversion. The final values for SBP and DBP were used as indicators to evaluate the efficacy of tai chi in the intervention group and control group. Some trials provided means of SBP and DBP, but did not provide SD, the SD of SBP and DBP were calculated using the following formulas: (i) if the number of samples (n) and the standard error (SE) were known, SD was calculated as:
SD = SE × √n;
(ii) estimates of SD were calculated if the number of samples (n), mean, and 95% CI (17–19) were known: “a” and “b” are the upper and lower confidence limits, respectively:
SD = a −mean /1.96 √n
SD = mean −b /1.96 √n.
Study selection
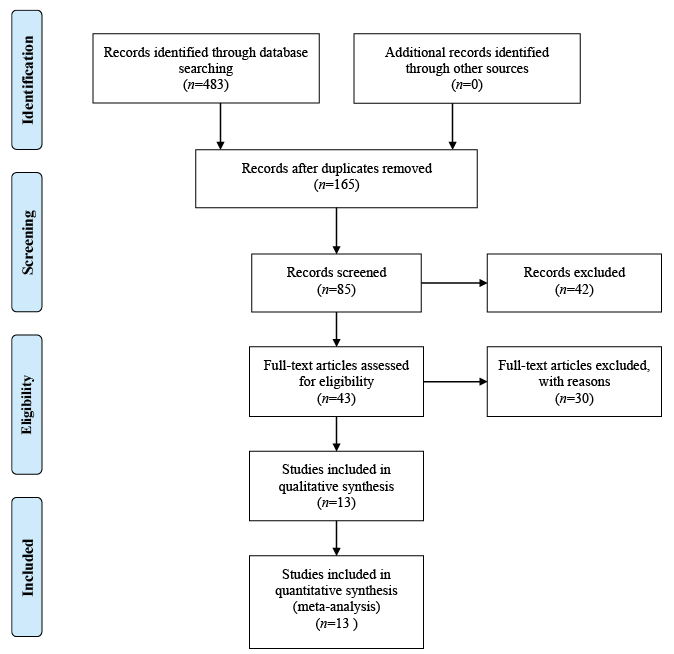
A total of 483 study reports were screened, 165 of which were excluded because they were duplicate publications. After reading the titles and abstracts, an additional 233 articles were excluded, and 85 articles retained. Among them, 42 articles did not meet the inclusion criteria, 16 studies did not have a suitable control group and, for 14 studies, the data could not be extracted. Finally, 13 RCTs, with a total of 1,461 participants, were included. The PRISMA flow diagram is shown in Fig. 1.
Fig. 1. Study selection procedure according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement.
Study characteristics
The principal characteristics of the studies are summarized in Table I. Thirteen studies were published between 1999 and 2018, which included a total of 1,461 participants. The number of participants in the individual studies ranged from 14 to 136. Seven of the included trials were single-centre studies. The included studies came from different countries: China (20, 21, 24, 25, 27–29, 31), Korea (22, 23), America (32), Switzerland (30) and Vietnam (26). The duration of the intervention varied from 6 to 48 weeks. All participants had essential hypertension. Four RCT trials (20, 23, 24, 29) used yang-style tai chi, 6 RCT trials (25–28, 30, 31) used 24-movements tai chi, and 3 RCT trials (21, 22, 32) used simplified tai chi and did not report the tai chi style.
Table I. Randomized controlled trials included in the systematic review on the effects of tai chi on hypertension
Quality assessment
Figs 2 and 3 provide an overview of the risk of bias for the included studies, based on the tools provided by the Cochrane Manual. All included studies used a double-blind approach and reported dropouts. Most trials reported allocation concealment and random allocation, but did not mention the specific method used. Eight studies (20, 25–31) reported automatic generation of random sequences by a computer, while 2 studies (23, 24) reported that they divided participants into an experimental group and a control group by using random number tables. Selective reporting was unbiased, but without any description to evaluate the existence of other biases. All the included trials reported whether or not adverse events occurred.
Fig. 2. Risk of bias graph: review authors’ judgements about each risk of bias item presented as percentages across all included studies.
Fig. 3. Risk of bias summary: review authors’ judgements about each risk of bias item for each included study.
Systolic blood pressure
Fig. 4 shows the forest plots of the SBP analysis. The number of RCTs included was 13. The combined result was statistically significant (WMD = −6.58, 95% CI (−8.14, −5.02), p = 0.005), and tai chi had a positive effect on SBP in patients with essential hypertension compared with the control group. A random effects model was used for the quantitative SBP data and still showed heterogeneity (I2 = 60%, p < 0.0001).
For SBP subgroup analysis, the intervention group was first divided according to the different tai chi training methods. The included studies all reported on the tai chi training methods; the 24-movement style tai chi was a simplified version of Yang-style tai chi, which classified the 2 methods into 1 category, while the remaining simplified tai chi styles, which were not explicitly reported, belonged to another subgroup. The subgroup analysis was performed according to different durations of tai chi intervention: ≤ 12 weeks and > 12 weeks. For the interventions with a duration ≤ 12 weeks, (20, 23, 24, 27, 31), the combined results of the 5 studies showed that 24-movements or Yang-style tai chi did significantly reduce SBP (WMD = −6.79, 95% CI (−9.90, −3.69), p < 0.0001), with high heterogeneity (I2 = 44%, p = 0.15) (Fig. 5). In the intervention duration > 12 weeks group (25, 26, 28–30), the combined results of the 5 studies also showed that 24-movements or Yang-style tai chi significantly reduced SBP (WMD = −5.90, 95% CI (−8.73, −3.06), p < 0.0001), with high heterogeneity (I2 = 53%, p = 0.10) (Fig. 5). During the intervention durations ≤ 12 weeks (21,22,32), the combined results of the 3 studies showed that other types of simplified tai chi did not significantly reduce SBP (WMD = −4.77, 95% CI (−13.84, 4.31), p = 0.3), with high heterogeneity (I2 = 72%, p = 0.03) (Fig. 6). However, for the intervention durations > 12 weeks, no studies fit this category.
Fig. 4. Forest plot of the comparison of the mean systolic blood pressure in 13 randomized control trials of the effect of tai chi on essential hypertension.
Fig. 5. Forest plots comparing 24-movements or yang-style tai chi, with subgroup analysis according to different intervention durations, with the systolic blood pressure (SBP) results of the control group.
Fig. 6. Forest plots comparing other simplified styles of tai chi, with subgroup analysis according to different intervention durations, with the systolic blood pressure (SBP) results of the control group.
Diastolic blood pressure
In terms of reducing DBP, there was a significant difference between the tai chi group and the control group (SMD = −0.57, 95% CI (−0.77, −0.37), p < 0.0001) (Fig. 7). There was substantial heterogeneity among the included studies (I2 = 69%, p = 0.0001).
For analysis of the DBP subgroup, due to the different types of tai chi included in this meta-analysis, the 24-type tai chi and Yang’s tai chi were classified into a single subgroup and the rest of the tai chi categories into another subgroup. The durations of studies with 24-movement or Yang-style tai chi were all ≤ 12 weeks (20, 23, 24, 27, 31). The combined results of the 5 studies comparing 24-movement or Yang-style tai chi with a control group showed significant differences (SMD = −0.84, 95% CI (−1.06, −0.61), p < 0.00001), with low heterogeneity (I2 = 0%, p = 0.72) (Fig. 8). The intervention durations in studies with 24-movement or Yang-style movements were all > 12 weeks (25, 26, 28–30). The combined results of the 5 studies comparing 24-movement or Yang-style tai chi with a control group showed a significant difference (SMD = −0.51, 95% CI (−0.72, −0.30), p < 0.00001), with high heterogeneity (I2 = 58%, p = 0.05) (Fig. 8). The combined results of 3 studies showed that other styles of tai chi did not significantly reduce DBP (SMD = −0.38, 95% CI (−1.44, 0.67), p = 0.47) with intervention durations ≤ 12 weeks (21, 22, 32); these studies had high heterogeneity (I2 = 83%, p = 0.02) (Fig. 9).
Fig. 7. Forest plot of the comparison of the mean diastolic blood pressure in 13 randomized control trials of the effect of tai chi on essential hypertension.
Fig. 8. Forest plots comparing 24-movements or yang-style tai chi, with subgroup analysis according to different intervention durations, with the diastolic blood pressure (DBP) results of the control group.
Fig. 9. Forest plots comparing other simplified styles of tai chi, with subgroup analysis according to different intervention durations, with the diastolic blood pressure (DBP) results of the control group.
Total cholesterol and triglycerides
Four included trials (22, 27–29), which included 476 participants, reported data on total cholesterol (TC) changes after practising tai chi. There was significant heterogeneity in TC between the patients with essential hypertension who participated in the tai chi intervention ant the patients in the control group (I2 = 94%, p < 0.00001). TC levels decreased in the tai chi group compared the control group, but there was no significant difference (SMD = −0.29, 95% CI (−0.73, 0.15), p = 0.20) (Fig. 10). Three studies (27–29) reported triglyceride (TG) levels in 448 patients, of whom 224 went through a tai chi intervention. There was relatively low heterogeneity among the 3 studies (I2 = 1%, p = 0.36). There was a significant difference in TG levels between the essential hypertension patients who received a tai chi intervention and the control group (WMD = −0.19, 95% CI (−0.22, −0.16), p < 0.00001) (Fig. 11).
Fig. 10. Forest plot of the comparison between tai chi and the control group for the outcome total cholesterol (TC).
Fig. 11. Forest plot of the comparison between tai chi and the control group for the outcome triglycerides (TG).
High- and low-density lipoproteins
Four included RCT trials (20, 27–29) with a total of 612 participants provided data on blood high-density lipoprotein (HDL) levels. There was highly significant heterogeneity among the 4 studies (I2 = 94%, p < 0.00001). The level of HDL in the tai chi group was higher than in the control group, but the difference was not significant (SMD = 0.59, 95% CI (−0.12, 1.29), p = 0.10) (Fig. 12). Low-density lipoprotein (LDL) levels were reported in 3 trials (27–29) with a total of 448 participants. There was low heterogeneity among the 3 studies (I2 = 0%, p = 0.60). There was a significant difference in LDL between the essential hypertension patients who received a tai chi intervention and the control group (WMD = −12.55, 95% CI (−15.96, −9.14), p < 0.00001) (Fig. 13).
Fig. 12. Forest plot of the comparison between tai chi and the control group for the outcome high-density lipoprotein (HDL).
Fig. 13. Forest plot of the comparison between tai chi and the control group for the outcome low-density lipoprotein (LDL).
Body mass index and waist circumference
Seven included trials (21, 25, 26, 28–30, 32) with 1,039 participants reported data on changes in body mass index (BMI) after practising tai chi. There was highly significant heterogeneity among the 7 studies (I2 = 96%, p < 0.00001). BMI decreased in the tai chi group compared with the control group, but the difference was not statistically significant (SMD = −0.11, 95% CI (−0.75, 0.52), p = 0.73) (Fig. 14). Four included studies (23, 25, 28, 29) with 638 patients reported changes in waist circumference (WC) after tai chi practice. There was relatively high and statistically significant heterogeneity among the 4 studies (I2 = 61%, p = 0.05). There was a significant difference in the WC between the essential hypertension patients who received a tai chi intervention and the control group. (WMD = −0.37, 95% CI (−0.63, −0.10), p = 0.006) (Fig. 15).
Fig. 14. Forest plot of the comparison between tai chi and the control group for the outcome body mass index (BMI).
Fig. 15. Forest plot of the comparison between tai chi and the control group for the outcome waist circumference (WC).
Publication bias
The publication bias of the 13 RCTs was evaluated with a funnel plot and found to be small (Fig. 16).
Fig. 16. Funnel plot of 13 randomized control trials on the effect of tai chi on essential hypertension.
Tai chi originated from ancient eastern traditional culture, and its development has absorbed traditional philosophy, the theory of yin and yang, the theory of the 5 elements, the theory of meridians and other traditional Chinese theories. It is widely used, and, as a form of low-intensity aerobic exercise, it is increasingly popular in terms of health. Previous studies have revealed that practising tai chi can increase the central excitability of breath and aspiration, the excited focus spread to the parasympathetic nerve, parasympathetic excitability, and peripheral small pulse relaxation, and reduce spasms, blood flow resistance, and BP (9). Tai chi has the coordinated effect of regulating the heart, body and breath, which produces a relaxation effect, reduces hyperactivity of the sympathetic nervous system, corrects the imbalance of the nervous system, and improves symptoms of hyperactivity of the sympathetic nervous system, such as dizziness and neck tension. However, previous clinical research conclusions have been inconsistent. Meanwhile, in previous systematic reviews, the possible impact of different tai chi training durations and styles has not been evaluated. Through quantitative synthesis, this study found that tai chi, as a physical exercise, seems to be effective in controlling BP in patients with essential hypertension, and suggests that different training durations and methods have different therapeutic effects.
Summary of the main results
Combined with the current research results, we found that tai chi is effective in treating essential hypertension. This systematic review and meta-analysis showed that the effects on SBP and DBP in the tai chi intervention group were stronger than those in the control group. There was heterogeneity in the reduction of SBP and DBP, but significant differences in the effects were observed. Subgroup analysis of SBP showed that there was a significant decrease in SBP with practising 24-movement or yang-style tai chi for ≤ 12 weeks or > 12 weeks. However, the results also showed that other simplified types of tai chi did not significantly decrease SBP when the intervention duration was ≤ 12 weeks, and the heterogeneity among the studies was higher.
There was a significant difference in DBP reduction between those who practised 24-movement or yang-style tai chi and the control group. However, other types of simplified tai chi did not significantly reduce DBP and the studies had high heterogeneity. Our research is the first to notice that different training durations and styles of tai chi intervention may lead to different effects. The results show that 24-movement or yang-style tai chi had effectiveness in reducing SBP or DBP, after a duration of either ≤ 12 weeks or > 12 weeks. However, when the duration was ≤ 12 weeks, other styles of simplified tai chi had no effect on reducing SBP and DBP.
The current study also focused on hypertension risk factors (BMI, TC, TG, WC, HDL, and LDL). Tai chi was found to have a beneficial effect in studies that reported TG, LDL, and WC levels. Studies have shown that the cerebral cortex is in a “relaxed” state when practising tai chi, which is a state of protective inhibition that can reduce the excitability of the sympathetic nervous system, leading to a decrease in norepinephrine and epinephrine, which, in turn, can reduce vasoconstrictive enzyme activity. During tai chi, the tissue is stimulated to release histamine, irritants and other substances, which relaxes the blood vessels and reduces BP (13). One study showed that tai chi promoted health, prevented disease, and had a positive effect on arterial stiffness and static/dynamic balance (15). Some studies have shown that tai chi can enhance the use of active neural networks by regulating physical and psychological methods (14).
Study limitations
This study has several limitations. First, in some cases, we had to calculate and transform data, rather than these being provided directly. Secondly, the study distribution between the 13 RCTs was included; most studies were conducted in Asian countries, such as China (Taiwan) or Korea, which may affect the meta-analysis results. The results of the included studies showed significant differences, which may be due to inconsistent exercise intensity. A sensitivity analysis of the included RCTs found that 2 studies may be a source of most of the heterogeneity. In both studies, the study design was a single-centre study with a small number of participants, which may have an impact on the comprehensive measurement results. In addition, language and publication biases limited our study. Finally, this review included only randomized controlled trials. There is a need for more diverse research, such as into the cooperation between multiple centres, more rigorous clinical reports, and prospective studies.
Clinical implications
BP is well known to fluctuate as the result of complex interactions between external environmental and behavioural stimuli, intrinsic cardiovascular regulatory mechanisms, humoral influences, and rheological factors. Far from being a background noise or a phenomenon occurring at random and able to dilute the prognostic value of the mean BP measurements, BP variability is a reproducible measure (33). Furthermore, there is accruing evidence that high variability in BP is a major vascular risk factor and a determinant of target-organ damage (34–36). As tai chi reduces hyperactivity of the sympathetic nervous system and corrects the imbalance of the nervous system, which can have a significant role in determining BP variability, it would be of great interest to investigate the effect of tai chi on variability of BP levels over time.
This study summarizes the current status of research into the effect of tai chi in patients with essential hypertension and provides data to support future clinical trials of essential hypertension. Although this study shows that tai chi can effectively control BP levels in patients with essential hypertension, due to the low quality of these research methods and the observed clinical heterogeneity, the current evidence and potential findings should be interpreted with caution. Cerebral haemodynamics are often impaired in patients with hypertension, a cause of brain dysfunction, and it is noteworthy that it is reversible (37). In view of the current research, it is also valuable to explore the effect of tai chi on cerebral vasomotor response (38). Taking into account the mechanism of action of tai chi, it is possible that tai chi may also have favourable effects on the immune system and affect the systemic inflammatory status. A growing body of evidence suggest that individual inflammatory status can be assessed through easily available serum biomarkers (39, 40). The effect of tai chi on inflammatory biomarkers should be evaluated in future studies. This would also increase our understanding of the effects and potential longer-term benefits of tai chi, not only on BP, but on other metabolic parameters.
Conclusion
Tai chi is an effective physical exercise intervention in patients with essential hypertension compared with control interventions. Different training durations and styles of tai chi have different effects. Further RCTs with rigorous study designs are needed to determine the efficacy of tai chi in the treatment of essential hypertension and its risk factors, and to investigate its use in healthy lifestyle interventions to prevent or treat essential hypertension and other related chronic diseases.
This project was supported by the National Key Basic Research and Development Plan of China (2011CB505406) and the Basic Research on Health Identification of Traditional Chinese Medicine in Tianjin Colleges and Universities “Innovation Team Training Plan” (approval number TD13−5049) during the 13th 5-year plan period. The authors thank Professor Huaien Bu for providing important information.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize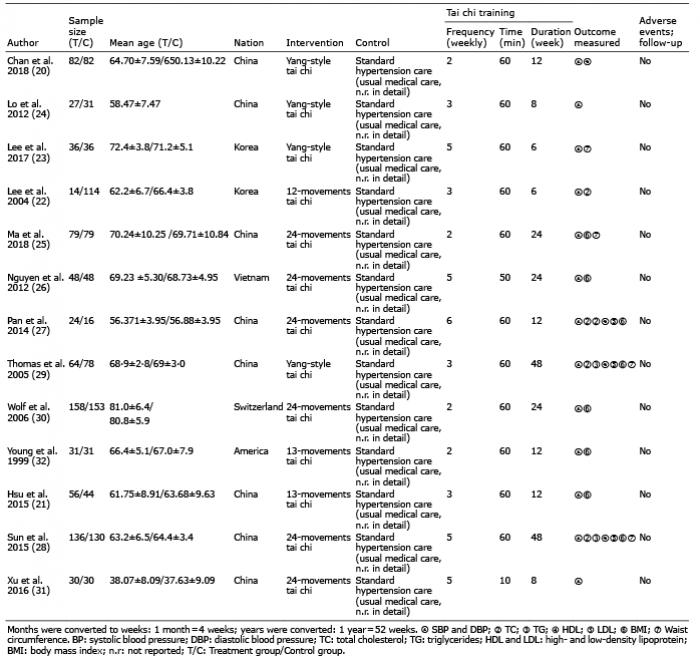 Click to show fullsize
Click to show fullsize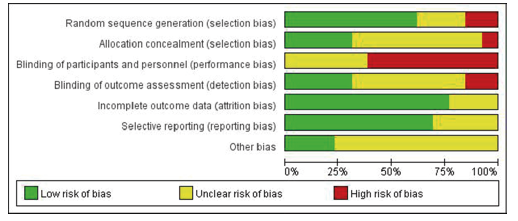 Click to show fullsize
Click to show fullsize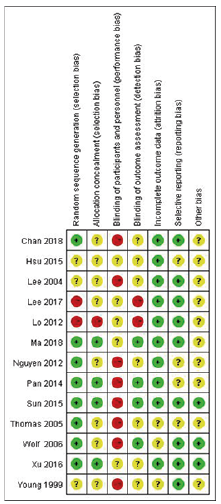 Click to show fullsize
Click to show fullsize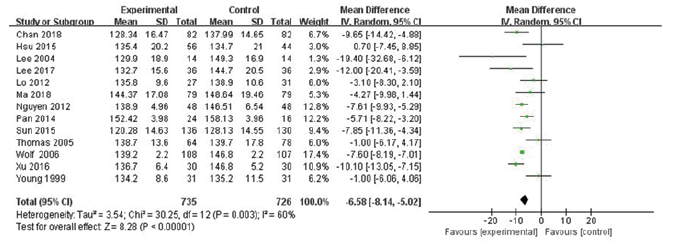 Click to show fullsize
Click to show fullsize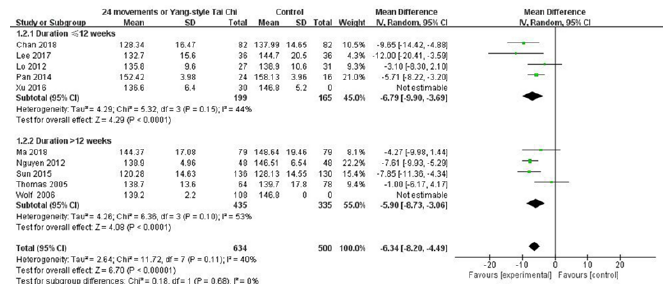 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize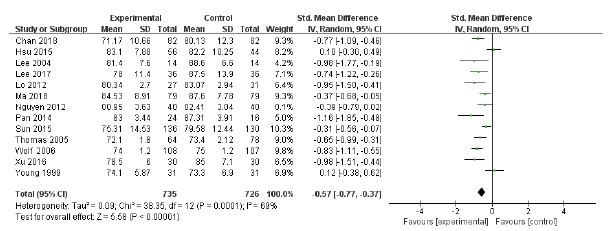 Click to show fullsize
Click to show fullsize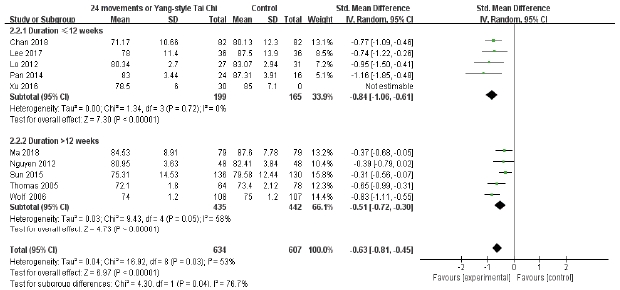 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize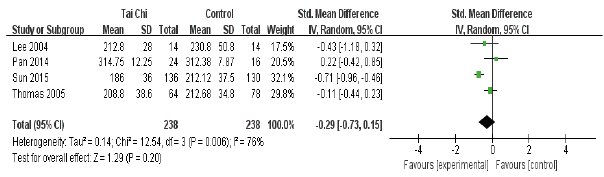 Click to show fullsize
Click to show fullsize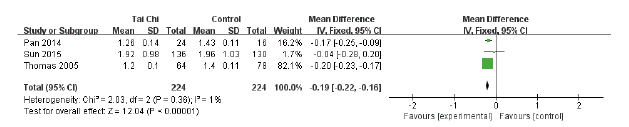 Click to show fullsize
Click to show fullsize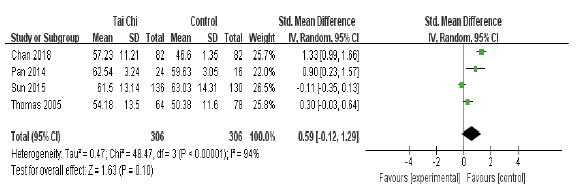 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize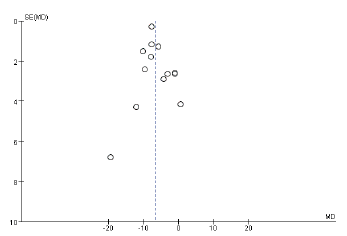 Click to show fullsize
Click to show fullsize